
STARRS Position
STARRS believes that serving is a privilege, not a right, and that potential recruits and officer candidates need to meet the physical and mental standards required to fight our nation’s wars.
Unit readiness, unity and deployability are essential to effective mission accomplishment.
An individual with gender dysphoria and seeking medical treatment for transitioning to a different sex does not meet this criteria and is an unnecessary financial burden.
Thus, STARRS does not support the DoD policy on this matter.
DoD Policies
Current DoD policy, DoDI 1300.28, states that transgender service members (SM) are allowed to receive gender dysphoria “treatments” as determined necessary by a physician. This includes psychological evaluation and counseling and “transition” hormones and surgeries, paid for by the taxpayers.
Transgender personnel will meet dress, appearance and fitness standards, be assigned berthing, use bathrooms and locker rooms, etc. in accordance with their gender marker in the Defense Enrollment Eligibility Reporting System (DEERS). Their gender marker can be changed in DEERS once the prescribed medical treatment is complete and they are “stable.”
With the approval of a military doctor, “transition” can be deemed “complete” without surgical removal or alteration of body parts. If the treatments do not resolve the gender dysphoria or associated concerns, the service member can be “transitioned” back to their “original gender”.
Long-term exceptions to policy can be granted for fitness standards, such as body mass index (BMI), due to the impact of hormone treatments.
The Center For Military Readiness points out that the DoD instruction does not allow for the protection of rights of religious liberty for chaplains and people of faith who object to the transgender ideology on moral grounds.
Nor does it provide any options for doctors, nurses, and other medical personnel who do not want to participate in “transgender treatments” that violate personal convictions or medical ethics.
Instead, commanders will be held accountable if anyone in their chain of command uses the “wrong” pronouns or makes any statement that might be construed as “biased against transgender individuals.”
STARRS’ Analysis
Bottom Line:
There is a long list of medical, psychological, physiological and intelligence factors that disqualify people from serving based on their ability to execute the mission, including age, weight, height, physical disability, medical conditions (asthma, heart conditions, epilepsy, color blindness, some dental conditions, hearing damage, history of food allergies, etc.), depression, bipolar disorder, anxiety disorder, drug additions, criminal history, inability to pass the physical fitness test, lack of a high school diploma or equivalent, inability to achieve the minimum score on recruitment exams, etc.
The DoD policy does not consider the realities of human DNA and biological science. Changes in outward appearance do not change biological realities.
There is a shortage of reliable scientific data on the long term effects of “gender-affirming” treatments, but science indicates they have a low success rate and result in the need for long-term care and significant negative impacts on the ability of the service member to effectively execute mission requirements.
DoD policy ignores religious freedom and medical ethics, and makes no allowance for those with strong religious and moral objections to aspects of transgenderism.
“Gender transition” medical treatments adversely impact the military and VA budgets due to the high cost of surgeries and life-long hormone treatments, mental health counseling, and medical care for chronic conditions resulting from “gender transition” surgeries.
- It is feasible that people will join specifically to get these services at no cost to them, yet not be able to maintain standards and fully carry out their duties.
There is a significant negative impact on readiness due to individual duty limitations during and after “gender affirmation treatments” and the diversion of funds from other priorities.
Expending funds allocated for national defense should not be used to facilitate medical procedures that are medically and culturally controversial.
The trans agenda is an integral part of the international Marxist and globalist movements and is changing the culture on military bases for the worse.
Detailed Discussion
1. Policy Concerns
The DoD policies do not account for the realities of human DNA and biological science. Changes in outward appearance do not change biological realities.
These mandates violate minimal expectations of personal privacy in close quarters, and deny the realities of human emotions and behavior, including sexual attractions and the desire for personal modesty between men and women. In multiple places DoDI 1300.28 states variations of:
“For facilities subject to regulation by the military, service members will use those berthing, bathroom, and shower facilities associated with their gender marker in DEERS.”
The instruction does not allow for individual beliefs (religious, secular or science) that are contrary to the policy. This includes chaplains and medical personnel.
The new policy ignores historical DoD data and an in-depth analysis conducted by Secretary of Defense James Mattis and a panel of experts in 2017-2018 that led to the policy implemented by President Trump. The panel studied the results of President Obama’s transgender policies. In a letter to President Trump, Secretary Mattis concluded:
“…there are substantial risks associated with allowing the accession and retention of individuals with a history or diagnosis of gender dysphoria and require, or have already undertaken, a course of treatment to change their gender”…and that…“exempting such persons from well-established mental health, physical health, and sex-based standards…could undermine readiness, disrupt unit cohesion,, and impose an unreasonable burden on the military that is not conducive to military effectiveness and lethality.”
When asked about transgenders in the USAFA cadet wing, cadets related:
- There was a female cadet that sought to “transition.” Her roommate was okay rooming with her. However, after “transition surgery”, the roommate no longer wanted to room with the surgically altered cadet. Male cadets did not want to room with the altered cadet either. Does this mean that the cadet should get a private room?
- “The last thing I want to do is shower with a cadet who is transitioning.”
- “Most of the time we’d rather focus on training that affects all of us rather than the <1%. For all of us to give up our valuable M5 (military training hour, 5th period on M-days/every other academic day) time which is usually a whole hour after lunch, just to be more inclusive will frustrate cadets and honestly just make them less receptive. Sometimes it feels like we are just bonding over how much we don’t like our time being wasted and we can unite behind the dislike for unnecessary training.”
DoDI 1300.28 and 6400.11 restricts research into and the release of data related to transgender policies without the approval of the Under Secretary of Defense for Personnel and Readiness (USD(P&R)), thus hiding the information from the rest of the government and the public, and preventing oversight and re-evaluation based on analysis of actual impacts over time.
In particular, 6400.11 paragraph 5.3.d.6.a.2: “A certificate of confidentiality prohibits disclosing or providing information created or compiled for purposes of research in any federal, State, or local civil, criminal, administrative, legislative, or other proceeding.”
2. Medical data: There is a absence reliable scientific data on the long term effects of “gender affirming” treatments, but science indicates they have a low success rate and result in the need for long-term care.
Dr John Hughes, MD and STARRS participant, states “A big concern is a scarcity of medical data on long-term effects; worse in kids, but definitely increased risk of stroke, heart disease and blood clots.”
The The Heritage Foundation reports that the largest dataset on sex-reassignment procedures—both hormonal and surgical—reveals that such procedures do not bring the promised mental health benefits. With some conditions, the problem got worse.
In a letter published in the Wall Street Journal, a group of endocrinologists stated: “Every systematic review of evidence to date, including one published in the Journal of the Endocrine Society, has found the evidence for mental-health benefits of hormonal interventions for minors to be of low or very low certainty.” The letter stresses that the risks of life-long sterility and medical dependency, as well as continued mental trauma, have greater certainty than the little-supported evidence in favor of “hormonal transition.”
The Daily Mail in the UK reported that a Portland “gender-affirming” surgeon admitted in a now suppressed video that patients face a lifetime of infertility, incontinence and sexual dissatisfaction. The video also discusses “high maintenance,” intensive aftercare, difficulties in using their new genitalia for pleasure and how the doctors in the field are “developing” surgical and after-care strategies. They are learning as they work cases.
3. Mental Health Concerns: Mental conditions that make it hard to deploy are normally disqualifying.
The US Army admits that people with gender dysphoria experience mental health issues. According to an Army Sustainment Command Public Affairs article in US Army, common mental issues of LGBTQ people include depression, suicidal thoughts, shame, fear, stress, etc. In fact, they state that the risk of depression, PTSD and suicidal ideation is twice their non-LGBTQ peers.
This article concludes that “gender-affirming treatments” reduce this risk, but other studies disagree. To some extent the article bases this conclusion on the case of one US Army major (who now goes by Rachel Jones) who has “transitioned” and who is highlighted in the article. No other references are used to substantiate the claim that treatments help.
Data analysis by the Society for Evidence Based Gender Medicine (SEGM) led to their conclusion that the mental health needs of people suffering from gender dysphoria are significantly greater than those of the general population and surgeries don’t change that.
According to a CMR policy analysis service members with gender dysphoria were found to be eight times more likely to attempt suicide than service members as a whole (12% vs. 1.5%)
The Heritage Foundation reports that largest dataset on sex-reassignment procedures—both hormonal and surgical—reveals that such procedures do not bring the promised mental health benefits.
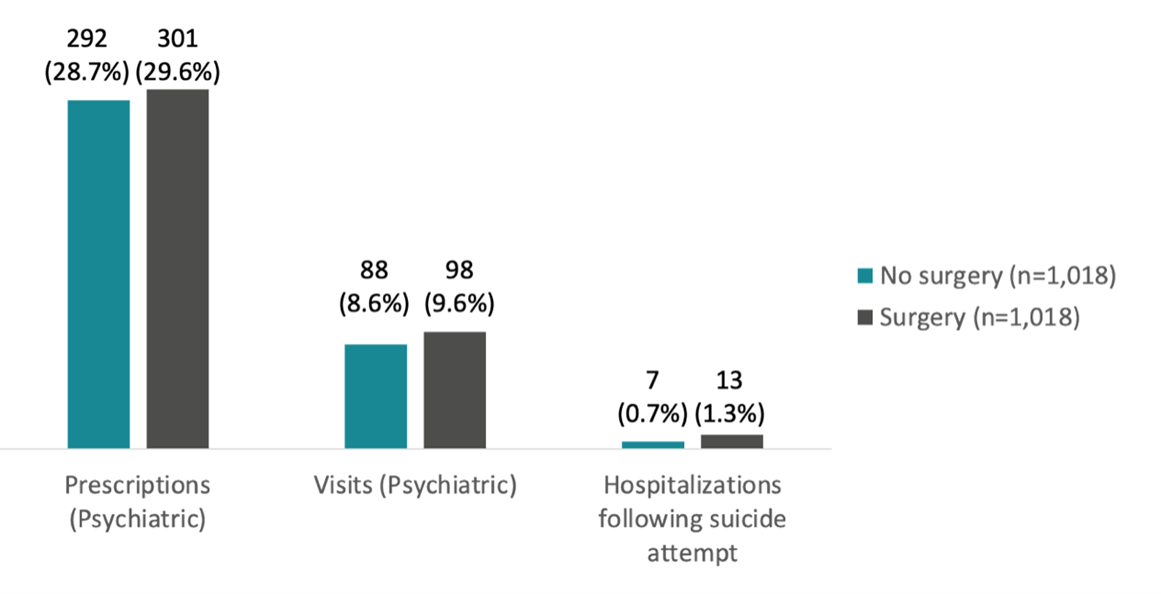
- Treatment for anxiety disorders: individuals diagnosed with gender incongruence” who had received “gender-affirming” surgery were more likely to be treated for anxiety disorders compared with individuals diagnosed with gender incongruence who had not received “gender-affirming” surgery.
- A clinic would need to perform 49 surgeries before they could expect a single patient to benefit.
- Such surgeries can have deadly consequences. The Centers for Medicare and Medicaid Services pointed out: “The study identified increased mortality and psychiatric hospitalization compared to the matched controls. The mortality was primarily due to completed suicides (19.1-fold greater than in control Swedes).” These results are tragic, and they directly contradict the most popular media narratives, as well as many of the snapshot studies that do not track people over time. Indeed, the Obama administration noted that “mortality from this patient population did not become apparent until after 10 years.”
People are coming forward trying to tell their stories about how they came to believe they needed to “transition,” what it was like, their later regrets, and their current challenges with “de-transitioning” after irreparable surgeries and other treatments. Trauma is an effective way to describe what they go through.
– Chloe Cole’s story: Chloe describes her journey, including the role of social media and a culture that looks negatively on females, especially traditional roles like being a mother. Dr Jordan Peterson explains the psychology of growing up as it applies to her experiences.
– Interview with Dr Miriam Grossman, a psychologist who works with people with gender dysphoria. She has written books and speaks about the history of the gender ideology and the devastating impact it’s having on youth and their families. She also touches on the science that shows the biological differences between males and females are far more then genitalia, the differences go as deep as organs and the vast majority of the cells, and it all makes a difference in all bodily functions (this is discussed starting around 1:20).
Epoch TV Cross Roads reports that a neuropsychologist and military veteran, Alan Hopewell, says there is the potential for those on hormone treatments to become more aggressive and that the hormones will affect their overall mental stability. With the stress of being deployed, this could be a problem. A recent Danish study (late June 2023) points out a high mortality rate due to suicide. Mr. Hopewell points out that there has been a lack of studies into the impacts of these medications. What treatment and support will be needed by service members on these treatments in field or deployed environments where access to medical care is extremely limited? Transgender service members have reported that they are referred off-base for their care because of a lack of expertise on-base. This is not possible in a deployed environment.
The “So What” Factor (why does this matter): Can the average service member count on fellow service members dealing with mental confusion/instability to have their back and do the right thing during life-threatening and stressful combat situations?
4. Budget impact: Expending funds allocated for national defense should not be used to facilitate experimental medical procedures that are culturally controversial.
In June 2021 military.com reported that over the previous five years (2016- early 2021) the Pentagon spent $15 million treating 1,892 transgender troops. Of this $11.5 million went for psychotherapy and $3.1 million for surgeries. As large as these numbers seem, it included a period (2018 – Jan 2021) during which the Trump Administration had enacted a policy barring individuals with gender dysphoria from serving, with exceptions. Transgender individuals who did not have gender dysphoria were allowed to serve in their “birth gender.” It can be assumed that since the Biden Administration overturned the Trump policy five days after taking office that costs have increased, but we have yet to find the data.
A CMR policy analysis reports that in February 2018 a panel of experts compiled data that showed from 1 October 2015 to 3 October 2017:
- 994 active-duty service members diagnosed with gender dysphoria accounted for 30,000 mental health visits.
- Medical costs for service members with gender dysphoria, usually involving hormone treatments, increased nearly three times — or 300%.
Major “transition” costs, including expensive hormone treatments, will be paid for by the government (DoD and later VA) for life. According to a July 2019 article in Mount Sinai “transition” costs for a single patient frequently exceeds $100,000 in the civilian sector.
DoDI 1300.28 states “A Service member who has completed a gender transition but has not resolved the gender dysphoria should consult with their military medical provider and commander. If a return to their previous gender is medically required, the Service member is to use the procedures outlined in Paragraph 3.4. of this issuance.” This means that defense dollars will be used for even more expensive treatments and surgeries in an attempt to fix previous misjudgments of a patient’s gender identities.
We have found no evidence that these expenditures will improve military readiness or morale in the All-Volunteer Force.
5. Readiness Impact
Numerous related expenses will put a strain on a unit’s budget, adversely impacting the ability of units to send service members to training and mission-related TDYs.
Service members recuperating from “transition surgery” will be on convalescent leave and limited duty for extended periods of time, requiring others to take up the slack/fill in. Units are authorized a specific number of people based on mission requirements; there are no excess military members.
If there are complications, service members could require an indefinite amount of convalescent leave, not to mention costly, on-going medical expenses and duty limitations, and potentially VA service-connected disability payments and care for life.
The hormone treatments result in significant increases in Body Mass Index (BMI) in men “transitioning” to women, requiring exceptions to fitness standards. Overweight service members are unable to complete physically demanding tasks and have increased risks for numerous physical ailments common in the obese, further limiting duty performance and increasing the need for expensive medical care.

It is completely feasible that young people seeking to transition would enlist for the sole purpose of “transitioning” at U.S. taxpayer expense. While I’m the service, their duty availability will be limited and they will be non-deployable for major parts of their enlistment. After discharge, the Veterans Administration will have to pay for their life-long care.
6. Marxist and globalist ideological intention is to change American culture, with military culture change being a significant part of that.
The Trans agenda is an integral part of the international Marxist movement and is slowly changing the culture on military bases. Liz Wheeler explains the connection between Marxism and the trans agenda in an interview with Sebastian Gorka on 4 Aug, 2023. Read more in her book Hide Your Children, Exposing the Marxists Behind the Attack on America’s Kids.
The parent of a service member told STARRS that when asked about transgenders in the unit, the SM thought there could be three, but “I cannot talk about it, don’t ask anymore. I can get in serious trouble if I so much as get somebody’s pronouns wrong.” Marxist goal: control the narrative, intimidate and silence opposition.
During a presentation at the World Economic Forum’s 2022 annual meeting a representative from the WEF’s Power of Media Task Force discussed how they are a proud partner of Global LGBTQ Equality (also known as the Partnership for Global LGBTI Equality (PGLE)) which was launched at the WEF in 2019 in coordination with the UN High Commission for Human Rights.
She states that they work with the news, business, entertainment, faith leaders, sports, governments and activists to educate people on LGBTQ issues and move policy forward.
Those signing up for our military have already been indoctrinated during their K-12 education and the military is re-enforcing that indoctrination. An undercover video shows how New York educators strategically, quietly and disruptively incorporate gender based ideology into lesson planning and the classroom environment (rainbow stickers, banners, posters, language used, books read) to open kids minds to other opportunities and pathways.
Subtle tricks could be putting a picture of a nonbinary looking person on a math sheet. They can include LGBTQ examples along with common examples – “Hey, we’re gonna read a book from Dr. Seuss, here’s a quote from Martin Luther King, here’s a quote from RuPaul (dubbed the Queen of Drag; producer, host, judge of RuPaul Drag Race, a reality competition television series), and a quote from…”
As one educator said, “Just little drops of exposure throughout someone’s upbringing. That’s what settles into our psyche as what normal is….Those are the subtle things that I think make ripples that make waves.” Watch more.
K-12 DoD schools are not immune from pushing the agenda (article in The Federalist).

The military has been engaging in gender pronoun training for at least a couple years.
Military academies have LGBTQ clubs and awards/recognition, Transgender Awareness week, Transgender Visibility Seminars, etc.
Deceptive propaganda/disinformation is used to convince people that the lifestyles are normal, safe and a good thing. Marxist goal: control public opinion.
Hormone treatments and surgeries render patients infertile. Marxist and Global Reset goal: control and decrease the human population.
Affirming and celebrating the transgender movement undermines the value of the human family and religious faith. Marxist goal: degrade the human family and religion and replace them with the State.
Long-term impacts and the stories of people seeking to “de-transition” (but unable to completely go back to normal) are being suppressed by the US government, the medical community, big tech and the majority of the media. Marxist goal: control public opinion.
STARRS Position Paper on DoD Transgender Policies (PDF)
Recommended for expanded background information:
DoD Report and Recommendations on Military Service by Transgender Persons, February 2018, prepared by Secretary of Defense James Mattis and a panel of experts tasked with studying the issue; https://partner-mco-archive.s3.amazonaws.com/client_files/1521898539.pdf
CMR analysis The Trump/Mattis Transgender Policy – What Are the Facts; https://www.cmrlink.org/issues/full/the-trumpmattis-transgender-policy-what-are-the-facts
The Transgender Empire, How the Trans Movement Conquered American Life, Christopher Rufo; https://rufo.substack.com/p/the-transgender-empire
Discussion between two doctors that perform gender affirming surgeries, https://videos.dailymail.co.uk/video/mol/2023/07/14/4031759648158888168/640x360_MP4_4031759648158888168.mp4
Dr. Jordan Peterson’s interview with Chloe Cole, https://podcasts.apple.com/in/podcast/319-detransition-the-wounds-that-wont-heal-chloe-cole/id1184022695?i=1000591961656
Jordan Peterson’s April 2023 Interview with Dr Miriam Grossman, https://youtu.be/Su2Z4_iQHz4
References
DoD Instruction 1300.28, In-Service Transition For Transgender Service Members; https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/130028p.pdf
Letter from Secretary of Defense Mattis to President Trump with his recommendations resulting from an in-depth study of transgender service; https://partner-mco-archive.s3.amazonaws.com/client_files/1521897476.pdf
Biden Pentagon Quietly Expands Woke Transgender Policies in the Military, Center for Military Readiness, https://www.cmrlink.org/news-releases/full/biden-pentagon-quietly-expands-woke-transgender-policies-in-the-military
Correction of a Key Study: No Evidence of “Gender-Affirming” Surgeries Improving Mental Health; Society for Evidence Based Gender Medicine, Aug 30, 2020, https://segm.org/ajp_correction_2020
“Transitioning” Procedures Don’t Help Mental Health, Largest Dataset Shows, Ryan T Anderson, Ph.D., Aug 3, 2020. https://www.heritage.org/gender/commentary/transitioning-procedures-dont-help-mental-health-largest-dataset-shows
The Wall Street Journal; https://www.wsj.com/articles/trans-gender-affirming-care-transition-hormone-surgery-evidence-c1961e27?mod=opinion_major_pos16
The Daily Mail, United Kingdom, https://www.dailymail.co.uk/news/article-12299393/Portland-surgeon-dubbed-Dr-Frankenstein-reveals-drawbacks-genital-ops-trans-adolescents.html?ito=social-twitter_mailonline
Living Authentically Saves Soldier’s Life, US Army, https://www.army.mil/article/267818/living_authentically_saves_asc_soldiers_life
Correction of a Key Study: No Evidence of “Gender-Affirming” Surgeries Improving Mental Health; Allowing scientific debate in transgender medicine improves evidence basis, Society for Evidence Based Gender Medicine, https://segm.org/ajp_correction_2020
Physicians: Trans treatments for kids pushed in U.S. for political reasons, not medical evidence, World Tribune, 14 July 2023, https://www.worldtribune.com/physicians-trans-treatments-for-kids-pushed-in-u-s-for-political-reasons-not-medical-evidence/
Here’s How Much the Pentagon Has Spent So Far to Treat Transgender Troops, Military.com, 18 June 2021. https://www.military.com/daily-news/2021/06/18/heres-how-much-pentagon-has-spent-so-far-treat-transgender-troops.html
The Epoch Times, Cross Roads with Joshua Philipp, 7 July, 2023; https://www.theepochtimes.com/revealing-the-risks-with-americas-transgender-soldiers-darlene-sanchez-on-the-serious-side-effects_5381309.html
Primary Author of this Paper
 Col Tracey Meck, USAF (ret) is a 1987 graduate of the United States Air Force Academy. Upon graduation, she was assigned to the Security Forces career field and held numerous positions at the unit and higher headquarters level to include two Security Forces Squadron commands and Air Staff positions. She served as the Provost Marshal for JTF SHINING HOPE and JTF ATLAS RESPONSE. In 2005, she deployed to Bagram Air Field, Afghanistan, where she served as Deputy Commander, 455th Expeditionary Mission Support Group in support of Operation ENDURING FREEDOM for four months. From Apr 06 to Apr 07 she served as the Commander of Provincial Reconstruction Team Gardez where she was responsible for improving province and district-level governance capacity, security forces effectiveness, and selecting and conducting reconstruction projects throughout Paktya and Logar provinces in Afghanistan. In 2011, she served as the the Chief of Staff for the Iraqi Training and Advising Mission, Ministry of Interior. As the US military transitioned out of Iraq, she forward deployed to Djibouti in the Horn of Africa where she served a six month tour as the Chief Staff Officer for a Joint Task Force. She received her career field’s highest award, the Air Force Billy Jack Carter Award for the year 2000. This awarded is given to the person who made the most significant contribution to protecting Air Force personnel and resources during the award period. She has a master’s degree in organizational management from the University of Phoenix.
Col Tracey Meck, USAF (ret) is a 1987 graduate of the United States Air Force Academy. Upon graduation, she was assigned to the Security Forces career field and held numerous positions at the unit and higher headquarters level to include two Security Forces Squadron commands and Air Staff positions. She served as the Provost Marshal for JTF SHINING HOPE and JTF ATLAS RESPONSE. In 2005, she deployed to Bagram Air Field, Afghanistan, where she served as Deputy Commander, 455th Expeditionary Mission Support Group in support of Operation ENDURING FREEDOM for four months. From Apr 06 to Apr 07 she served as the Commander of Provincial Reconstruction Team Gardez where she was responsible for improving province and district-level governance capacity, security forces effectiveness, and selecting and conducting reconstruction projects throughout Paktya and Logar provinces in Afghanistan. In 2011, she served as the the Chief of Staff for the Iraqi Training and Advising Mission, Ministry of Interior. As the US military transitioned out of Iraq, she forward deployed to Djibouti in the Horn of Africa where she served a six month tour as the Chief Staff Officer for a Joint Task Force. She received her career field’s highest award, the Air Force Billy Jack Carter Award for the year 2000. This awarded is given to the person who made the most significant contribution to protecting Air Force personnel and resources during the award period. She has a master’s degree in organizational management from the University of Phoenix.